yussimania
Surgery, Roids and Raw Milk
Glossary:
MPA - Mandibular Plane Angle
OP - Occlusal Plane
LAFH - Lower Anterior Facial Height
MMC - Maxillomandibular complex
CCW - Counter Clockwise
CW - Clockwise
JFA - Jaw Frontal Angle
For Frontal profile:
The reason we rarely see people ascend frontally is less to do with rotation - the most important thing is vertical movements of the maxilla (downgraft or impaction) which allows for more rotation and advancement of the mandible. Also the Genioplasty when trimax cases are done which will affect your JFA and LAFH the most due to movement in both sagittal, vertical and transverse planes. Ramus Widening can increase the bigonial width.
Gonial angle/MPA changes:
Gonial angle changes are limited you will never achieve a "rotational morph" where the entire MMC rotates due to OP limits and the type of cut for the BSSO and Lefort.

The standard cut for BSSO is the type C. This is anterior to the ramus and gonion which are key landmarks to the gonial angle. So now we need to change the relationship between the gonion and the menton however normal advancement with the standard few degrees of rotation won't change the MPA and thus gonial angle.
So here is my idea; GO BIG OR GO HOME. The more advancement you have the longer the lever and therefore wider the arc it travels during rotation. So if someone has severe sfs - a large advancement of say 20mm at the pogonion will yield far greater rotational results than your basic BSSO for your standard recession. By this logic we can see peoples gonial angles actually change for once.

Note the step off at the highlighted area due to the CW rotation - the gonial angle now has improved greatly increasing his LAFH.
But if we advance too much you risk being antefaced - remember we want the convexity profile (pogonion-subnasale-nasion or glabella) at around 175° +- 5°.
So this is very situational - if you don't have a vertical excess or deficiency - don't expect gonial angle to change during bimax; opt for implants or jawline shaving instead.
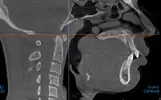
For Hyperdivergent profiles:
If your MPA and OP are close together then you will have some benefits with rotation - for example downswung people with a downward tilted MPA and OP when they have a Bimax advancement with CCW rotation and impaction their MPA will generally improve and theoretically will improve the gonial angle - however this is theoretical as I haven't personally seen a result yet.

See how the OP and MPA are closely related - this allows for more CCW rotation during bimax.
MPA - Mandibular Plane Angle
OP - Occlusal Plane
LAFH - Lower Anterior Facial Height
MMC - Maxillomandibular complex
CCW - Counter Clockwise
CW - Clockwise
JFA - Jaw Frontal Angle
For Frontal profile:
The reason we rarely see people ascend frontally is less to do with rotation - the most important thing is vertical movements of the maxilla (downgraft or impaction) which allows for more rotation and advancement of the mandible. Also the Genioplasty when trimax cases are done which will affect your JFA and LAFH the most due to movement in both sagittal, vertical and transverse planes. Ramus Widening can increase the bigonial width.
Gonial angle/MPA changes:
Gonial angle changes are limited you will never achieve a "rotational morph" where the entire MMC rotates due to OP limits and the type of cut for the BSSO and Lefort.
The standard cut for BSSO is the type C. This is anterior to the ramus and gonion which are key landmarks to the gonial angle. So now we need to change the relationship between the gonion and the menton however normal advancement with the standard few degrees of rotation won't change the MPA and thus gonial angle.
So here is my idea; GO BIG OR GO HOME. The more advancement you have the longer the lever and therefore wider the arc it travels during rotation. So if someone has severe sfs - a large advancement of say 20mm at the pogonion will yield far greater rotational results than your basic BSSO for your standard recession. By this logic we can see peoples gonial angles actually change for once.
Note the step off at the highlighted area due to the CW rotation - the gonial angle now has improved greatly increasing his LAFH.
But if we advance too much you risk being antefaced - remember we want the convexity profile (pogonion-subnasale-nasion or glabella) at around 175° +- 5°.
So this is very situational - if you don't have a vertical excess or deficiency - don't expect gonial angle to change during bimax; opt for implants or jawline shaving instead.
For Hyperdivergent profiles:
If your MPA and OP are close together then you will have some benefits with rotation - for example downswung people with a downward tilted MPA and OP when they have a Bimax advancement with CCW rotation and impaction their MPA will generally improve and theoretically will improve the gonial angle - however this is theoretical as I haven't personally seen a result yet.
See how the OP and MPA are closely related - this allows for more CCW rotation during bimax.
Last edited: